Patch Testing- Being a Skin Allergy Detective
This month I started offering patch testing in the clinic. Patch testing is a specialized type of testing to determine if itching or rash is coming from something that a patient is coming into contact with. Everyone seems familiar with the allergy testing that allergists do. They do blood tests or skin prick tests, usually for pollen, foods, dander, etc that causes hay fever and sinus troubles. That type of testing really doesn’t reveal anything about skin sensitivities. The vast majority of dermatitis (skin rashes that look like eczema) come from contact dermatitis to things our skin comes into contact with like fragrance, parabens, preservatives, dyes, resins, rubber products, metals… These reactions are mediated by delayed type hypersensitivity which can’t be evaluated using blood tests. Instead, we have to do provocative testing in which we apply these compounds to the skin and leave them in place, usually for 48 hours. (The allergists have it so easy with their simple skin prick testing and blood testing!)
I had sorely missed this diagnostic tool, but I hadn’t realized just how much. As a resident at Mayo, patch testing was one of many powerful tools that I had access to. Over decades, Mayo Dermatology had built up a vast library of nearly 700 substances that we could use to determine if a patient’s rash came about because of an allergy to something they came in contact with. There was a standard series of 80 things and then supplemental libraries of things for special situations like machinists, florists, dental hygienists, metalworkers, foot rashes, eyelid rashes, rashes in or around the mouth, bakers….
Out in the “real world,” this testing is largely unavailable. Its deemed too tedious and not lucrative enough to offer in the clinic (cuts into time they’d rather spend injecting Botox). If any type of patch testing is performed, it is usually with something called the TRUE Test, which is a simple screen for 36 allergens. At Mayo, we made fun of the TRUE Test because we would see patient after patient with a rash who was screened with the TRUE Test and deemed to not be allergic to anything becaues the TRUE test didn’t find anything. Not only did we often prove their rash was from an allergy, but many times we found that their allergy was to something that was actually part of the TRUE test, but that it failed to detect. In my first job after residency, I had to use the TRUE Test for the first time. I tested all kinds of people that I KNEW were allergic to something, but TRUE Test couldn’t find it. We’d have to either give up the hunt, or I’d have to refer the patient to someone who did real patch testing. I grew to despise the TRUE test, but since I worked for a big medical corporation it wasn’t my decision what was offered to patients.
Soon after opening my own practice, I was rapidly building up a list of patients that I KNEW had to be allergic to something, but how was I going to find it? TRUE Test is easy to do, but my previous experience validated the disdain we had for it at Mayo. I was not going to offer a test to my patients that I thought was a colossal waste of their time and money.
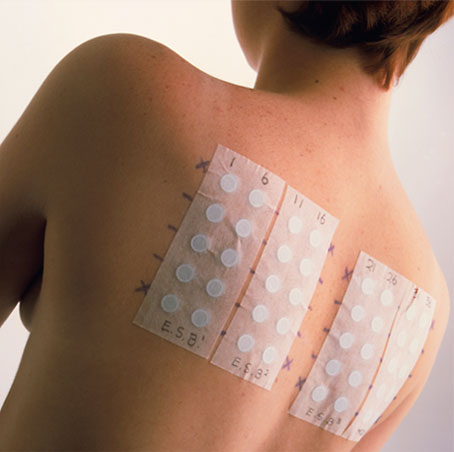
Patch testing is not simple. To do it right, (not with crappy TRUE Test) we have to take the compounds that we want to test and fill small chambers one-by-one and then apply those chambers to a patient’s back. To do testing with the North American Standard Series of allergens, this means setting up 70 chambers. These can’t be set up in advance. The test allergens are kept refrigerated in little syringes that need to be brought up to room temperature and then dispensed into the chambers on the day of the test. You have to be meticulous in organization because it is essential that you don’t foul up the order of the compounds and mix up what is in which chamber. So, after you fill 70 chambers with 70 different samples of test goo on the day of the test, you have to apply the chambers to the patient’s back. This is done on a Monday. They go home with this and can’t get them wet or sweaty. They come back on Wednesday for their removal and the first reading. Only 75% of reactions show up at 48 hours. Another reading on Friday will detect another 25% of reactions, but some of the reactions from the Wednesday reading will fade so you will miss those if you don’t do both readings.
The options were to refer them to a patch test specialist in downtown Seattle or to invest the time and resources to provide this service in my clinic.
That was an easy decision. We now have a starting library of 70 allergens in our medical refrigerator and I’ve taught my medical assistants how to setup the testing. Since I was taught to do it right or do it twice, we bring patients back for a 48 hour and a 96 hour reading.
The system I chose to implement is proving to be every bit as good as the system that I had access to at Mayo. This is going to let us help a lot of people. As examples, here are the stories of the first 3 patients who have gone through this testing:
- A gentleman in his 30’s who can’t wear deodorant because of the irritation it causes. He also has a 10 year history of sensitivity to fragrances, but this doesn’t explain his deodorant problem because he even has trouble with fragrance free deodorant. His patch testing shows that in addition to a ragingly severe allergy to fragrance, he also has allergies to a very large number of preservatives. This gives him the information that he needs to find products without these allergens that he ought to do fine with.
- A woman in her 50’s who has a really annoying rash around her neck. She is one of many people (we all know one) who can’t wear cheap jewelry. But, she stopped wearing necklaces and the rash persisted anyway. Patch testing confirmed an allergy to nickel (underlies about 90% of jewelry allergy), but also showed an allergy to lavender oil. Turns out she loves lavendar oil. But her love for lavendar oil isn’t enough for her to not give it up, which should lead to complete resolution of her rash. She didn’t react to ylang ylang oil. Maybe its time for her to go through a ylang ylang oil phase? But I’ll stick with what I know, and leave her next fragrance choice up to her.
- A gentleman in his 40’s who just itches. Kind of all over. Not severely, but a little bit, most days, and it has been going on for 6 months. No real cause can be found. Stopped various medications and supplements to see if they were the problem. Had no effect. Still itchy. If you had this for a week, you’d think no big deal, but after 6 months, it starts to drive you a little crazy. I wasn’t really sure that contact allergy was going to find the answer, but I recommended that we proceed with testing to rule it out. Sure enough, he’s allergic to all kinds of things.
Solving these mysteries is fun!
***UPDATE*** Since I originally wrote this blog post, we have tested dozens of patients and found all sorts of allergies. We have added new allergens, and we now have 79 unique allergens and 80 testing samples. I still love patch testing just as much! – Dr. Miller


No Comments
Sorry, the comment form is closed at this time.